In modern vascular medicine, we’ve come a long way. The introduction of endovascular aortic repair (EVAR, TEVAR, FEVAR, BEVAR, etc.) has transformed the treatment of complex aneurysms, dissections, aortic traumatic injuries, and penetrating ulcers. We now deploy stent grafts through small groin punctures instead of thoracotomies. We reconstruct visceral branches without a scalpel. We can even reline the aortic arch without cardiopulmonary bypass.
But for all our progress, one fundamental truth remains:
We are treating a manifestation, not a cause.
We are repairing an event in a disease that is still very much ongoing.
This is the concept of Progressive Aortic Disease, and it deserves more attention.
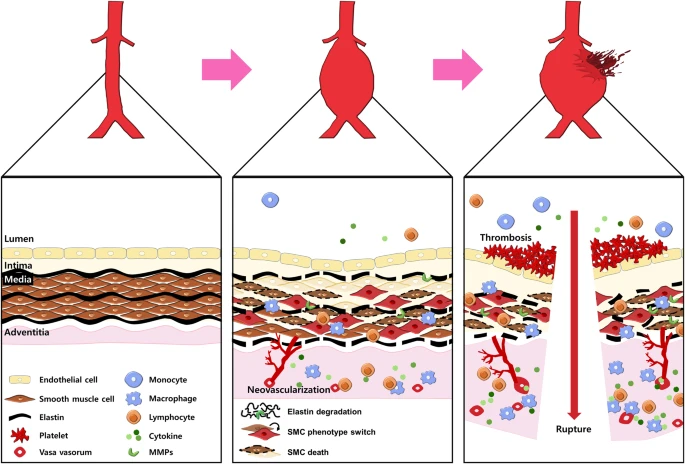
The aorta is not static plumbing. It is a dynamic, biologically active structure, constantly subject to the forces of:
With time, this biological machinery fatigues. What begins as segmental degeneration—an infrarenal aneurysm, a descending thoracic dissection—often continues beyond the treated segment. The pathology progresses, both proximally and distally, and even seemingly “normal” segments of the aorta can deteriorate over time.
This is not device failure. This is aortic disease progression.
It’s tempting to believe that newer generations of stent grafts, branched configurations, or improved sealing materials will somehow overcome the biological trajectory of disease. And while innovation is essential, it must be viewed as a tool, not a cure.
A beautifully executed FEVAR today may still face:
These are not procedural mistakes—they are expected outcomes in the life cycle of a progressively diseased aorta.
When we treat an aneurysm or seal a dissection flap, we interrupt a dangerous event. We protect the patient from rupture, malperfusion, or death.
But the aorta is still degenerating.
And unless we commit to a lifelong management model, we risk trading one catastrophe for another down the line.
Understanding the nature of disease progression allows us to anticipate some of the most common long-term complications:
These are not occasional complications—they are common realities of aortic disease as a living, progressive disorder.
Every aortic intervention should be viewed not as a solution, but as a chapter in a longer story. That story must include:
At Aortic Academy, we advocate for an end-to-end approach to aortic disease. Every procedure is an inflection point—but never the end point. The progressive nature of aortic degeneration demands that we build clinical pathways, device strategies, and team cultures that prioritize:
Because while technology enables us to repair an aorta today, biology determines what happens tomorrow.
Stay tuned for upcoming case-based modules and workshops on aortic surveillance strategies, long-term device performance, and integrated disease management pathways—designed for surgeons, interventionalists, and patients alike.