How to Launch a Total Endovascular Aortic Arch Repair Program: A Guide for Institutions
The evolution of endovascular aortic arch repair marks one of the most complex and technically demanding advancements in cardiovascular care. As outcomes improve and devices evolve, more centers are aiming to establish dedicated programs for total endovascular aortic arch repair (TEAAR). However, successful implementation requires more than just technical capability—it requires a highly coordinated system of care, proper infrastructure, experienced personnel, and institutional readiness.
At Aortic Academy, we’ve compiled this foundational guide to support hospitals, surgical centers, and academic institutions that wish to launch or formalize their own arch repair program.
1. Multidisciplinary Aortic Team
A successful arch program begins with a dedicated, collaborative team of subspecialists who manage complex aortic pathology from diagnosis through follow-up. At minimum, this team should include:
Vascular surgeons with experience in branched and fenestrated aortic procedures
Cardiac surgeons trained in arch surgery and comfortable with hybrid approaches
Interventional radiologists and cardiologists experienced in aortic imaging and endovascular navigation
Anesthesiologists trained in high-risk cardiovascular procedures with cerebral monitoring capability
Neurologists or neurointerventionalists for stroke risk management and pre-procedural evaluation
Intensive care specialists, perfusionists, and trained cath lab/hybrid OR nursing teams
A program coordinator or clinical manager to handle logistics, data, and multidisciplinary scheduling
This team must operate under structured clinical pathways, joint case reviews, and collaborative decision-making frameworks.
2. Physician Credentialing & Experience
Arch repair requires operators with significant experience in both thoracic endovascular aortic repair (TEVAR) and branched/fenestrated techniques. Institutional credentialing should require:
Documented case volume of complex aortic repairs (e.g. 25–50 TEVARs/year per operator)
Completion of device-specific training and proctored cases for branched arch devices
Familiarity with Zone 0–2 planning, cerebral protection strategies, and bailout conversion
Ongoing participation in case reviews, morbidity/mortality rounds, and registry contribution
Training and simulation programs—either in-house or through platforms like Aortic Academy—should support skill development.
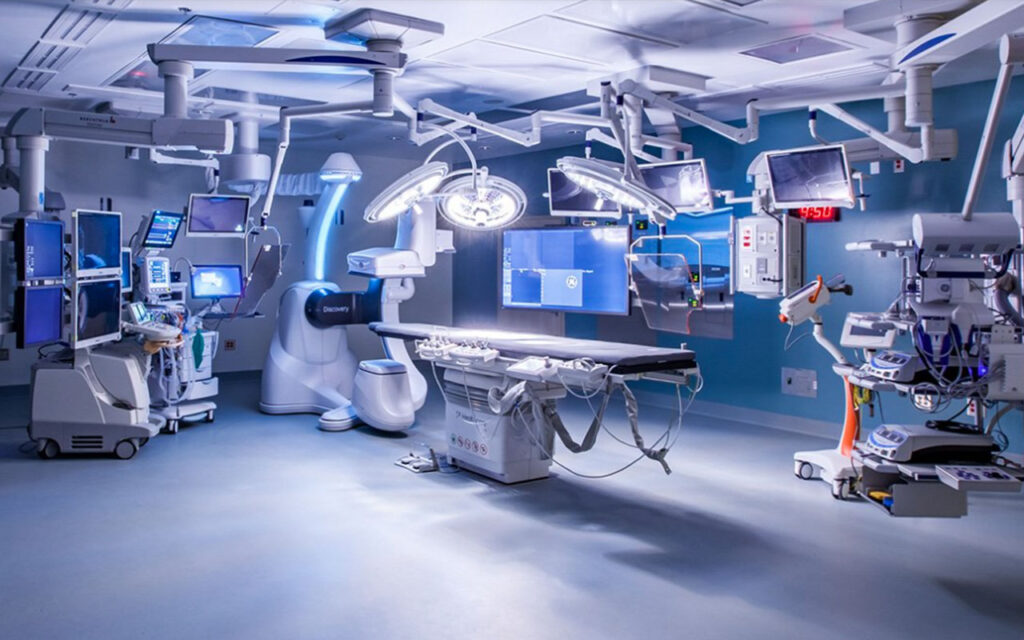
3. Hybrid Operating Room Standards
A hybrid OR or advanced angiosuite is essential for safe, image-guided arch interventions. Minimum infrastructure should include:
Fixed high-resolution imaging (preferably monoplane or biplane fluoroscopy with 3D overlay capability)
Table-compatible with radiolucent carbon fiber surfaces, tilt/rotation capability
Integration of image fusion, rotational angiography, and real-time measurements
Space to accommodate a full open and endovascular team including anesthesiology and perfusion
Backup open surgical equipment readily available (sternotomy instruments, CPB circuit, suction, etc.)
Centers without a true hybrid OR must evaluate whether mobile C-arms and portable setups meet imaging and sterility standards—most guidelines recommend fixed imaging for arch work.
Rapid access to cerebral embolic protection devices and stroke rescue equipment
Stocking and training staff on the use of contingency devices is equally critical (e.g. bare-metal stents, thoracic cuffs, chimney/snorkel strategies, and occlusion balloons).
5. Imaging & Preoperative Planning Requirements
Detailed anatomical assessment is a prerequisite for safe arch planning. Centers must have:
Access to high-resolution CTA with ECG-gating, 3D reconstruction, and thin-slice arch segmentation
Ability to perform centerline reconstructions and clock-face orientation of supra-aortic branches
Imaging software that allows planning for fenestration alignment, distance mapping, and angulation measurements
Preoperative assessment of Circle of Willis integrity and dominant vertebral artery via CTA or MR
Coordination with neurovascular and radiology teams for high-risk cerebrovascular anatomy
6. Anesthesia & Neuroprotection Standards
Aortic arch repair poses significant risk of cerebral ischemia and hemodynamic instability. Anesthesia protocols must include:
Cerebral monitoring tools such as bilateral near-infrared spectroscopy (NIRS)
Arterial line placement in both radial arteries (for detecting pressure gradients across arch vessels)
Transesophageal echocardiography (TEE) for wire and graft navigation
Rapid access to cardiopulmonary bypass (CPB) if emergent conversion is required
Ability to manage blood pressure augmentation or controlled hypotension as needed
Anesthesia teams must be specifically trained in aortic endovascular workflows, cerebral perfusion management, and crisis response.
7. Postoperative Care & Long-Term Follow-Up
Arch patients require meticulous post-op monitoring and structured imaging follow-up:
ICU team familiar with spinal cord perfusion, renal management, and stroke surveillance
Routine CTA at 1, 6, and 12 months, then annually
A dedicated outpatient aortic surveillance clinic
Documentation and integration into national or institutional aortic registries for quality control
Formal institutional approval through cardiac/vascular service lines
Development of standard operating protocols (SOPs) for case selection, emergency response, and discharge
Participation in peer-reviewed outcomes tracking, including 30-day mortality, stroke rate, endoleak rate, and reintervention
Collaboration with training platforms and societies (such as Aortic Academy) for continued professional development
Conclusion
Establishing a Total Endovascular Aortic Arch Repair program is a significant but achievable milestone for any high-level cardiovascular center. With the right team, imaging capability, hybrid infrastructure, and governance, institutions can elevate the standard of care for patients with complex aortic arch disease.
At Aortic Academy, we are proud to support centers worldwide in developing the technical, procedural, and strategic readiness needed to enter this field. Stay tuned for future workshops, simulation modules, and case-based proctoring tools to help your team move from vision to reality.
Legal Disclaimer
The content provided in this article and throughout the Aortic Academy platform is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment, nor is it intended to replace the clinical judgment of qualified healthcare professionals. All clinical decisions—especially those concerning patient care, procedural planning, or surgical interventions—must be made by board-certified and appropriately credentialed medical practitioners based on their own professional expertise, institutional protocols, and applicable regional regulations.
While every effort has been made to ensure the accuracy, currency, and relevance of the information presented, Aortic Academy makes no representations or warranties, express or implied, regarding the completeness, applicability, or clinical appropriateness of the content. We assume no responsibility or liability for any direct, indirect, incidental, or consequential harm, loss, or damage resulting from the use of any information or guidance provided herein.
Aortic Academy does not endorse any specific device, technology, or clinical approach mentioned unless explicitly stated, and any reference to commercial products or services is for educational illustration only. Readers are strongly encouraged to consult official guidelines, product IFUs, and institutional policies before implementing any technique or procedure discussed on this site.
Use of this website and its content constitutes agreement to these terms. For full legal terms, please refer to our Terms of Use and Privacy Policy.