In the world of advanced endovascular aortic interventions—where precision is paramount, the stakes are high, and every second counts—the importance of planning cannot be overstated. Operators are taught to enter the hybrid suite with a detailed procedural roadmap, encompassing primary and contingency strategies, access techniques, imaging protocols, and an exhaustive inventory of devices. But while strategy is critical, rigid adherence to the original plan in the face of shifting clinical realities can become a dangerous liability.
This is where the psychological concept of “Continuation Bias” enters the clinical realm—often quietly, but with significant consequence.

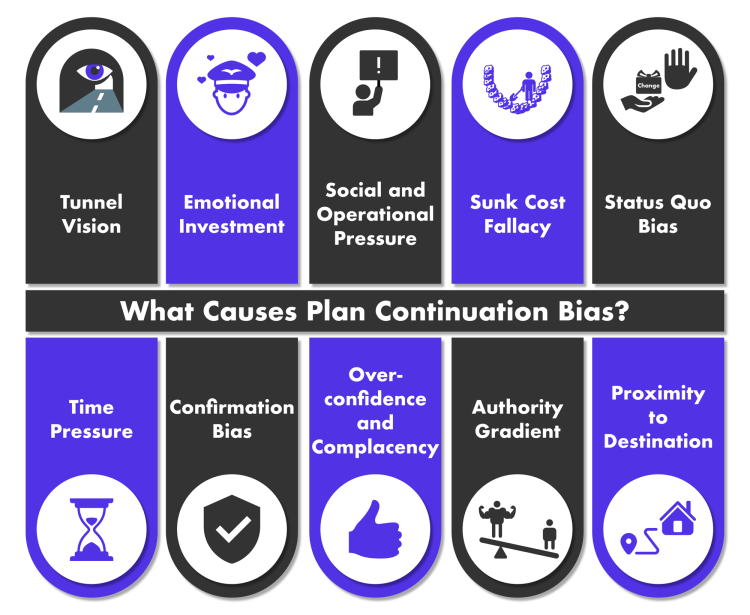
Continuation bias is a form of cognitive bias where individuals persist in a planned course of action, despite emerging evidence that suggests a change—or even cessation—is warranted. In aviation, it’s when a pilot insists on landing despite deteriorating weather or a malfunctioning system. In medicine, particularly during complex, prolonged procedures, continuation bias can manifest as:
These are not mere words. They are reflections of a very human tendency to avoid the discomfort of uncertainty, loss, or “giving up”—even when logic would dictate otherwise.
Endovascular aortic repair—especially in thoracoabdominal aneurysms, chronic dissections, and aortic arch pathology—demands deep pre-procedural planning. Experienced teams meticulously prepare for:
Yet despite best efforts, anatomy changes. Dissections occur. Wire access is lost. Patient physiology deteriorates. Devices behave differently than anticipated. The landscape shifts—and often so must the plan.
The ability to re-evaluate and pivot during a complex case is as important as technical skill itself. Here are key triggers that should prompt reassessment:
A new dissection, rupture, or access site injury may necessitate a radical deviation from the original plan. Pushing forward without adapting can amplify harm.
In prolonged procedures, even subtle changes in blood pressure, oxygenation, lactate, or urine output must be interpreted as warning signs—not afterthoughts.
Prolonged fluoroscopy times, repeated technical failures, and emotionally charged environments can drain decision-making capacity. Team exhaustion—especially in low-ventilated or overheated hybrid suites—can quietly erode judgment. This is when biases set in.
When operators begin “improvising” repeatedly or lose clear visualization of target vessels or graft positions, it may be safer to pause, stage, or abort.
The phrase “Live to fight another day” may sound cliché—but in the context of advanced endovascular repair, it’s a critical safety principle. Aborting a procedure is not a sign of failure; it is often a sign of wisdom, humility, and leadership.
In fact, staged interventions—with return to theatre once the patient is optimized, the anatomy stabilized, and the team recovered—often produce better outcomes than heroically “finishing” a case on the verge of collapse.
To reduce the impact of continuation bias, institutions and procedural teams can:
At Aortic Academy, we teach that preparation is the foundation of a safe and successful aortic procedure—but it’s adaptability and presence of mind that determine its true outcome. Every case is dynamic. Every team is human. And every moment in the hybrid suite carries an opportunity to pause, pivot, and protect the patient.
As we continue to push the boundaries of endovascular aortic repair, we must also push ourselves to recognize when the best decision is not to finish—but to stop, reflect, and re-engage with clarity.
Because the goal is not just to complete the procedure—but to preserve the life.